‘It is assumed that a person’s willpower defines their weight, but that is a big mistake’
According to María del Mar Malagón, obesity is a disease with multiple triggers, including gene mutations, endocrine disruptors and lifestyle habits


It is rare for a medical congress to make room for an event that departs from the usual round tables and major keynote speeches. Even less so, for the event to be a post-conference demonstration on, for example, precision medicine in obesity. But it does happen.
At its annual conference, the Spanish Society for the Study of Obesity (SEEDO) has scheduled a rally “in favor of people with obesity.” There is a lot to flag up, according to the president of SEEDO, María del Mar Malagón, 59 – starting with the basic fact that obesity is a full-blown disease, not a condition related to lifestyle, and including the need for awareness when tackling one of our century’s principle epidemics.
Malagón, who is also deputy scientific director of the Maimónides Institute of Biomedical Research in Córdoba and professor of Cell Biology at the University of Córdoba, has worked primarily in research. More specifically, she has focused on unraveling the secrets of adipose tissue, a structure that, despite its complexity and influence on obesity, has, she says, barely been considered worthy of a mention in the past. Now, things have changed, findings in obesity studies have multiplied and the condition is gradually gaining attention in the scientific community.
Question. Why is obesity not considered a disease?
Answer. Because it is assumed that a person’s willpower defines their weight, but that is a big mistake. This is part of the stigma and is one of the most erroneous concepts that exist right now concerning obesity, and that prevent it from being considered a disease. Even in scientific environments that are not specific to obesity, when I say that it is a disease, the general response is: “They should just keep their mouths shut.” And, of course, it is more complex than that.
Q. What is the origin of obesity?
A. There are multiple triggers. There are genes whose mutations determine the development of the disease [mutations in the leptin genes, for example], and there are other genes that make people susceptible to moderate or sequential weight gain. Other factors also have significant influence, such as our environment which not only encourages the consumption of hypercaloric food and drink, but ensures that food and drink will make us want to consume more. Together with a sedentary lifestyle, it all contributes significantly to the obesity epidemic.
Add to these factors, other environmental considerations, such as endocrine disruptors and lifestyle habits such as how many hours of sleep we get, which condition our weight through epigenetic mechanisms and accelerate weight gain. We also have conditions, such as mental illness, where the medication causes people to gain weight. Other factors that come into play include education, which reinforces eating habits, and purchasing power, which is also important. That’s why we propose a multi-faceted approach, because there are many types of obesity, defined by different combinations of these factors.
Q. What does it mean for a person to be obese?
A. Obesity is a significant risk factor when it comes to developing other chronic noninfectious diseases such as diabetes, cardiovascular and liver diseases, hypertension, certain types of cancer and, also, some mental illnesses. There is a high probability that obesity will be accompanied by these ailments. On a psychological level, people with obesity believe that it is their fault and that message is so terrible it can be read in their body language.
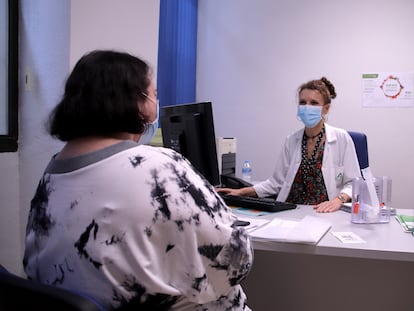
Q. The first thing you notice about a person with obesity is the excess weight. How important is the stigma?
A. It depends a lot on the person, but what a person with obesity goes through on account of having this disease and all that it entails is important; they feel ill, misunderstood and unable to control the disease. And knowing that you are not in control of the disease is terrible, as it generates anxiety.
Q. Does the public know what obesity entails, or does it trivialize it?
A. I don’t think they do know, and that is why we need to make ourselves heard. We have to change the paradigm. For example, until recently, carrying a few extra pounds was a sign of health and opulence, but that paradigm has to radically change.
Q. There is a movement called Health for Every Size that promotes the idea that a person with obesity can have still get good blood test results. Can an obese person be healthy?
A. This is a bit controversial. You can be healthy for a while, but it is only a matter of time before the excess weight causes problems. The risks accumulate with age. How long you stay healthy depends on your genetics and lifestyle, but we know what it can lead to. This does not detract from the fact that a person should be proud of their body the way it is. Their body is precious, but so is their health.
Q. Has treatment so far been all about getting the weight down?
A. Yes, absolutely. We have to change the paradigm and not only measure body mass index, but also body composition. There are thin people who have an accumulation of fat in the abdominal area. It is a question of fat distribution and muscle loss. And it is very important.
Q. One of the speakers at the congress discussed how fat tricks the brain. How does it do that?
A. Fat sends signals. It is like a sensor: when your fat deposit is full, hormones are sent to the brain as a signal of satiety, so that you stop eating. But, when it comes to obesity, this signal is short-circuited. Resistance is generated, you lose control and the signals that are sent are telling you to accumulate rather than burn fat.
Q. What alternative therapies are there for people with obesity?
A. Right now, not many. But there are good prospects for pharmacological treatment in the near future – between now and 2025. But with this complex disease, there are many parameters to control; as a large part of the organism is affected, we have to check that all aspects are controlled.
Q. Bariatric surgery is one of the procedures with the longest waiting list.
A. It is not prioritized. How available it is depends on the demand for other surgeries on a hospital’s organization chart. It is true that bariatric surgery has provided a solution for many people, but it also has complications. That is why I believe a multidisciplinary approach, including pharmacological treatments, would reduce this type of intervention which, although extremely good, is not advisable for all patients. We must focus on individualized treatment and have more therapeutic options.